


Public Comment to the FDA: Request for Suspension of mRNA-Based COVID-19 Vaccines
Disclaimer: This post is for informational purposes only and not medical advice. Always consult a qualified healthcare professional for medical concerns.

Dear FDA,
As a registered pharmacist and doctor of pharmacy, I urge the immediate suspension of mRNA-based COVID-19 vaccines (Pfizer-BioNTech Comirnaty, Moderna Spikevax) due to post-marketing evidence indicating that the risks outweigh the benefits. My own analysis, published on my Substack (https://substack.com/@danaiki) as well as in peer-reviewed literature, documents safety concerns that necessitate urgent regulatory action. (Banoun 2023, Seneff 2021 (Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19))
My article, Uncovering Concerns Surrounding mRNA Vaccines (Santiago 2025), references Banoun (2023), which highlights mRNA lipid nanoparticle persistence and potential DNA integration, suggesting that these products may function primarily as gene therapies rather than as traditional vaccines. My co-authored study, Oller and Santiago (2022), found a significant correlation between mRNA vaccinations and increased all-cause mortality in Public Health England data from 2021–2022. Additionally, VAERS reports and excess mortality data from Medicare and the EMA signal harm, including myocarditis and thrombotic events. (Kirsch 2023, Campbell 2023)
A complementary study by Levi et al. (2025), published as a preprint on medRxiv, examined 12-month mortality outcomes among 1.47 million matched Florida residents who received two doses of either Pfizer’s BNT162b2 or Moderna’s mRNA-1273 vaccine. The findings revealed significantly higher risks for Pfizer recipients across multiple endpoints:
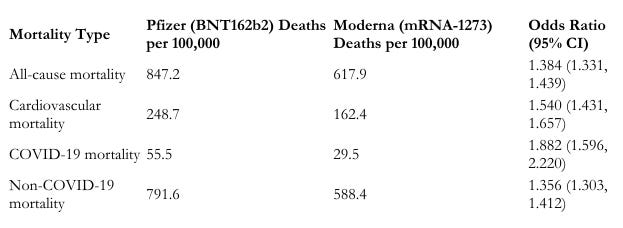
Despite meticulous matching for age, sex, race, ethnicity, vaccination site, and census tract, these differences persisted, reducing potential confounding factors such as healthy vaccinee bias. The study’s negative control outcomes, suicide and homicide deaths, showed no significant variation, reinforcing the reliability of the findings. Interestingly, these results contrast expectations, given that Moderna’s vaccine delivers roughly three times the mRNA content (100 µg) compared to Pfizer’s (30 µg).
Increased mortality risk was most pronounced in adults over 60, with cardiovascular and COVID-19 mortality curves diverging significantly after 30–200 days post-vaccination. These findings call attention to an urgent need for further investigation into differential risks associated with mRNA vaccines. See figure below

A preliminary forensic analysis of anomalous fibrin-like aggregates from postmortem human samples reveals hallmarks of abnormal protein aggregation, including enhanced autofluorescence, beta-sheet-rich domains, dense fibrillar ultrastructure, and spectral anomalies suggestive of pathological fibrin remodeling. (McCairn 2025) PCR confirmed a human origin, with preliminary evidence of molecular markers linked to recombinant spike protein exposure. (McCairn 2025) Despite limitations in sample provenance, these findings raise significant biosafety and pathophysiological concerns potentially related to SARS-CoV-2 and vaccine-induced spike protein effects, warranting urgent, controlled investigations to assess clinical and etiological relevance. The FDA’s approvals for mRNA vaccines relied on limited long-term data, and post-marketing surveillance now reveals risks that were not adequately addressed during Emergency Use Authorization or full approval reviews. I urge the FDA to take the following actions: 1. Suspend mRNA vaccine licenses pending an independent review of VAERS and global safety data. 2. Convene the Vaccines and Related Biological Products Advisory Committee (VRBPAC) to reassess the risk-benefit profiles of these products. 3. Mandate manufacturers to submit long-term biodistribution and genotoxicity studies within six months. Failure to act jeopardizes public safety and trust in FDA oversight. I request a written response to this comment and am available to provide further evidence.
Sincerely,
Daniel Santiago, RPh, PharmD

References
-Banoun H. mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues. Int J Mol Sci. 2023 Jun 22;24(13):10514. doi: 10.3390/ijms241310514. PMID: 37445690; PMCID: PMC10342157
-Kirsch, S. (2023a, February 9). EXCLUSIVE: Stunning new data pulled from the Medicare database shows how each shot increases your risk of death [Substack newsletter]. Steve Kirsch’s Newsletter. https://open.substack.com/pub/stevekirsch/p/exclusive-stunning-new-data pulled?r=11t26u&utm_medium=ios
-Kevin W. McCairn, Ph.D., Kevin McKernan Ph.D., Shojiro Kato M.D., Charles Rixey retired (USMC-CBRN). Cadaver “Calamari” Amyloidgenic Fibrin Aggregates, May 10, 2025, https://open.substack.com/pub/kevinwmccairnphd282302/p/cadaver-calamari-amyloidogenic fibrin?r=11t26u&utm_campaign=post&utm_medium=web&showWelcomeOnShare=false
- Levi, R., Mansuri, F., Jordan, M. M., & Ladapo, J. A. (2025). Twelve-month all-cause mortality after initial COVID-19 vaccination with Pfizer-BioNTech or mRNA-1273 among adults living in Florida. medRxiv. https://doi.org/10.1101/2025.04.25.25326460
-Oller, J. W., & Santiago, D. (2022). All cause mortality and COVID-19 injections: Evidence from 28 weeks of Public Health England “COVID-19 vaccine surveillance reports.” International Journal of Vaccine Theory, Practice, and Research, 2(2), 301–319. https://doi.org/10.56098/ijvtpr.v2i2.42
-Seneff, S., Nigh, G., Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19. (2021). International Journal of Vaccine Theory, Practice, and Research , 2(1), 38-79. https://doi.org/10.56098/ijvtpr.v2i1.23
Did you get a response?